Orange Peel Tea for Immune Support During these uncertain times, supporting your immune system and the microbiome is important. You can drink this tea throughout the day and swish it around your mouth (unsweetened) to support the oral and gut microbiome. Ingredients: Orange or any citrus peel (from 4-5 fruits)1/4 Onion1 inch Ginger2-3 Sprigs of Rosemary2 tsp Whole Cloves2-3 Star Anise1-2 tbs Fennel seeds 8-10 cups water. Bring to a boil & simmer for 20 minutes (or up to an hour) Keep in mind that you don’t have to have every single ingredient. There is no way to do this wrong. A simple tea of citrus peel is helpful. The other ingredients can be rotated. The goal is to use what you have on hand and get lots of polyphenols from these plants. Boiling these plants in water helps get the nutrients out. You can use a vegetable peeler to peel the citrus and save the peels in a bowl as you go in your fridge. Once you have enough, you can make tea. If you are having digestive issues, prioritize the ginger and fennel after the citrus peel. The onion provides quercetin, a flavonoid, useful for immune support, and is very antimicrobial. You don’t taste it in the tea, but it provides benefits. The spices all function to support the gut flora. Star anise contains shikimic acid and is used as a base material for the production of Tamiflu.
Cellular components of the organs and tissues, vascular and neurological structures are parts of tensegrity arrangement; Microbiome is an equal part of this ecosystem. Tensegrity is influenced by the microbiome. At the same time, mechanical properties of the connective tissue will influence microbiome composition and pathogenicity.
Cellular components of the organs and tissues, vascular and neurological structures are suspended in the tensegrity network and actually part of this network. Their form and function regulated by mechanical properties of the ecosystem they reside (Pre-stress).
Pre-stress is influenced by
microbiome and microbiome is regulated by pre-stress.
Microbiota are
ecological communities of commensal,
found in and on all multicellular organisms.
Microbiota includes bacteria, archaea, protists, fungi
and viruses. Microbiota have a crucial role
for immunologic, hormonal and metabolic
homeostasis of
their host. The synonymous term microbiome describes
either the collective genomes of
the microorganisms that reside in an environmental niche or the microorganisms
themselves
Microbiome
persist in nearly every human body site, including tissue and blood. The
genomes of these microbes continually interact with the human genome in order
to regulate host metabolism.
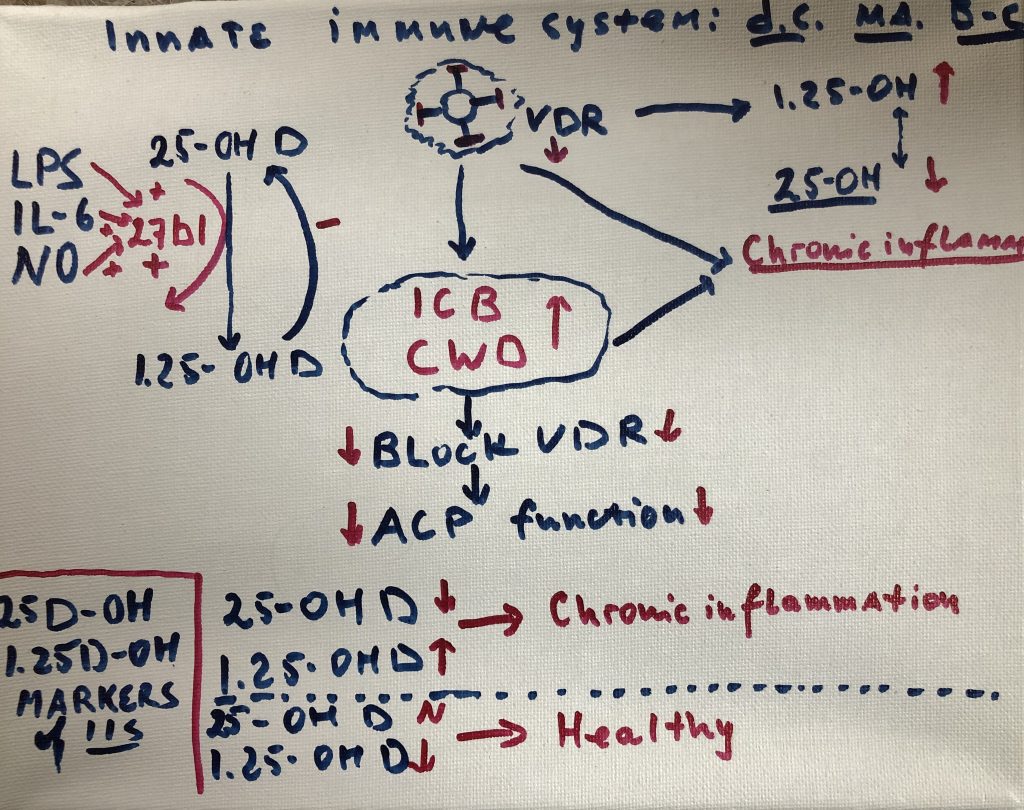
Many components of this microbiome are capable of both
commensal and pathogenic activity. This activity is determined by environment they
reside (viscoelasticity -pre-stress): immunological cells responsible for
innate and adaptive responses. They are additionally able to persist in both
“acute” and chronic forms. Inflammatory conditions historically
studied separately (autoimmune, neurological and malignant) are now repeatedly
tied to a common trend: imbalance or dysbiosis of these microbial ecosystems.
Collective activity of the
microbiome that drives inflammatory processes via complex microbe-microbe and
host-microbe interactions. Many microbes survive as polymicrobial entities in
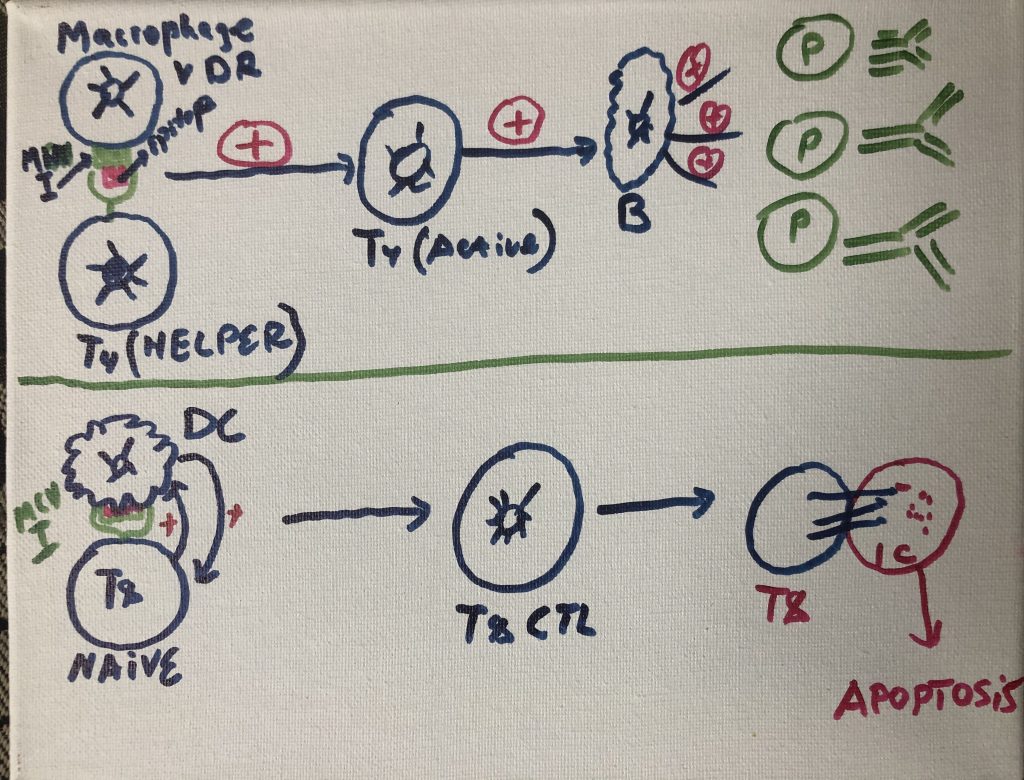
order to evade the immune response. Pathogens in these communities alter their
gene expression in ways that promote community-wide virulence. Other microbes
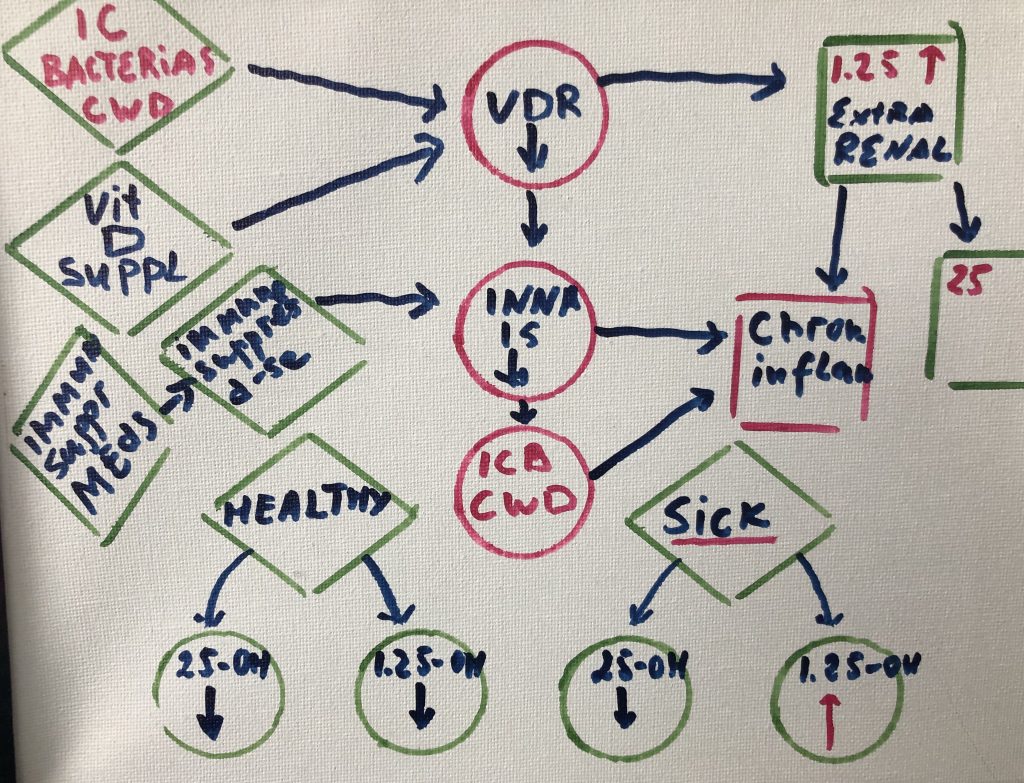
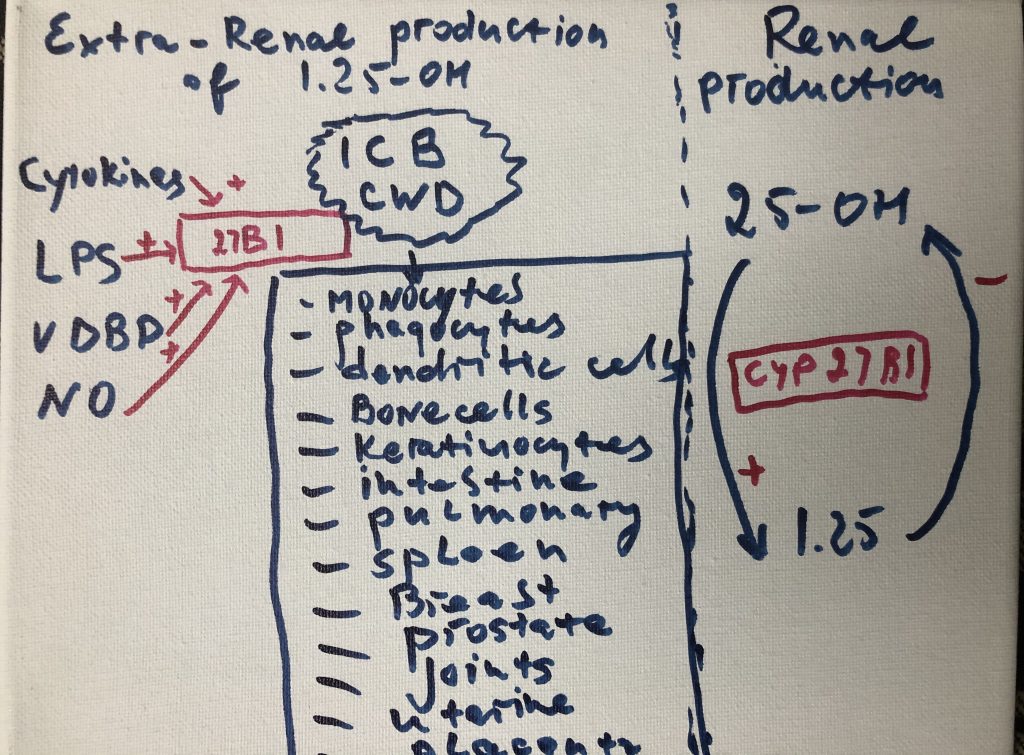
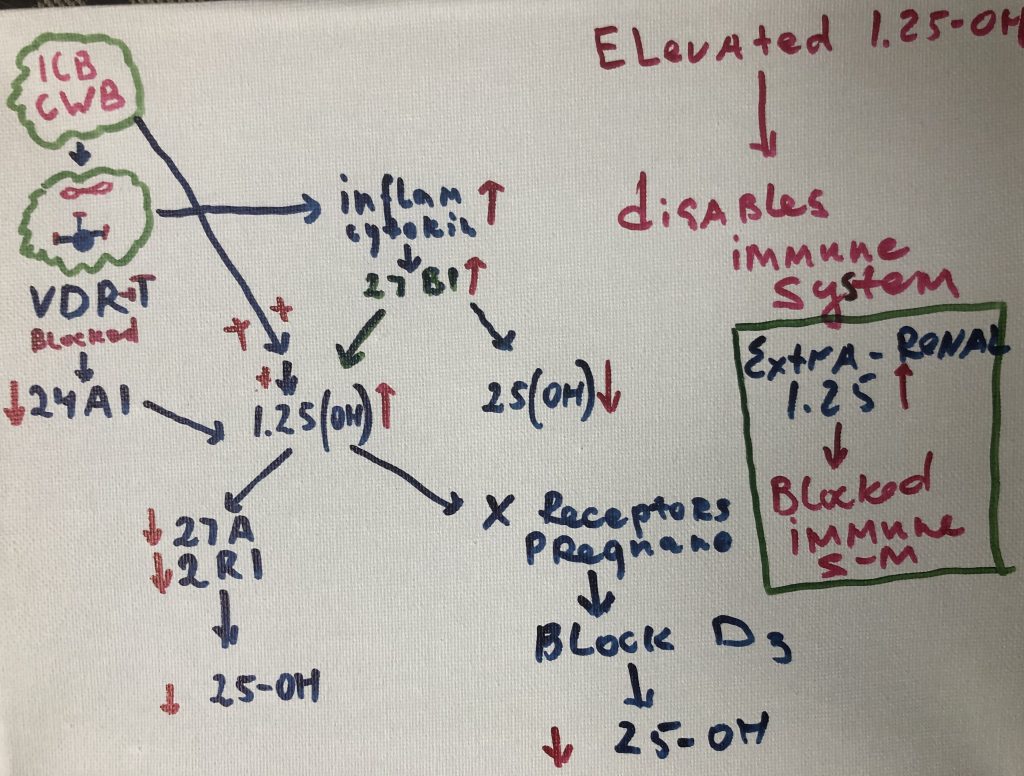
persist inside the cells of the immune system (Cell Wall Deficient bacteria -CWD),
where they directly interfere with host transcription, translation, and DNA
repair mechanisms. The numerous proteins and metabolites expressed by these
pathogens further dysregulate human gene expression in a manner that promotes
imbalance and immunosuppression. Molecular mimicry, or homology between host
and microbial proteins, complicates the nature of this interference. When taken
together, these microbe-microbe and host-microbe interactions are capable of
driving the large-scale failure of human metabolism characteristic of many
different inflammatory conditions.
Microbiota are “ecological communities
of commensal, symbiotic and pathogenicmicroorganisms” found
in and on all multicellular organisms. Microbiota includes bacteria, archaea, protists, fungi
and viruses. Microbiota have been found to be crucial for immunologic, hormonal
and metabolic homeostasis of
their host. The synonymous term microbiome describes
either the collective genomes of
the microorganisms that reside in an environmental niche or the microorganisms
themselves
Microbiome
persist in nearly every human body site, including tissue and blood. The
genomes of these microbes continually interact with the human genome in order
to regulate host metabolism.
Many components of this microbiome are capable of both
commensal and pathogenic activity. They are additionally able to persist in
both “acute” and chronic forms. Inflammatory conditions historically
studied separately (autoimmune, neurological and malignant) are now repeatedly
tied to a common trend: imbalance or dysbiosis of these microbial ecosystems.The collective activity of the microbiome that drives inflammatory processes via complex microbe-microbe and host-microbe interactions. Many microbes survive as polymicrobial entities in order to evade the immune response. Pathogens in these communities alter their gene expression in ways that promote community-wide virulence. Other microbes persist inside the cells of the immune system, where they directly interfere with host transcription, translation, and DNA repair mechanisms. The numerous proteins and metabolites expressed by these pathogens further dysregulate human gene expression in a manner that promotes imbalance and immunosuppression. Molecular mimicry, or homology between host and microbial proteins, complicates the nature of this interference. When taken together, these microbe-microbe and host-microbe interactions are capable of driving the large-scale failure of human metabolism characteristic of many different inflammatory conditions. (Amy D Proal)
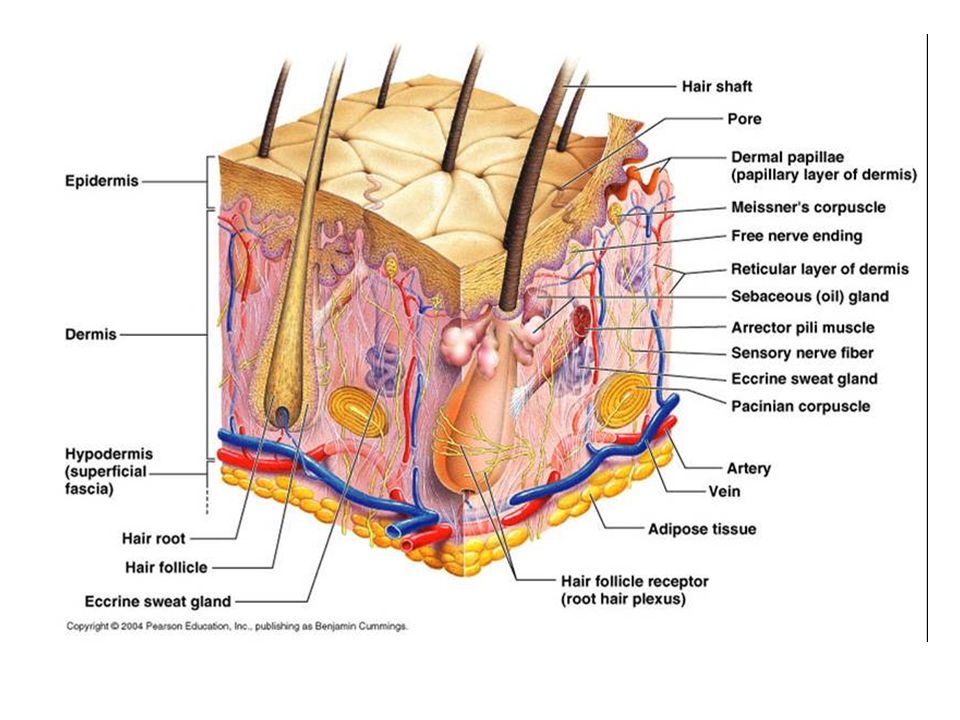
Mechanical properties of the skin are changed with time. Altered pre-stress changes first defenses of the immune system-physical barriers-Epidermis and dermal layers of the skin. Reduced functional capacity and increased susceptibility of the skin with development of dermatoses such as dry skin, itching, ulcers, dis-pigmentation, wrinkles, fungal infections, as well as benign and malignant tumors are the most common skin conditions in aged population. In turn altered appearance, dry skin, chronic wounds, and other conditions decrease general health and reduce the likelihood for healthy and active aging. Ability of the skin to carry out multiple and wide-ranging roles is very closely related to its structure, which is composed of an outer epidermis overlying an inner dermis, separated by a basement membrane.
Biochemical barriers: acidic, hydrolipidic nature of the
skin, as a result of sweat, sebum, lipids, and antimicrobial peptides
(AMPs).Any changes in lipid composition and epidermal differentiation lead to a
disturbed skin barrier, which plays a role in the pathogenesis of several
immune-mediated skin pathologies, such
as atopic dermatitis and ichthyosis vulgaris .
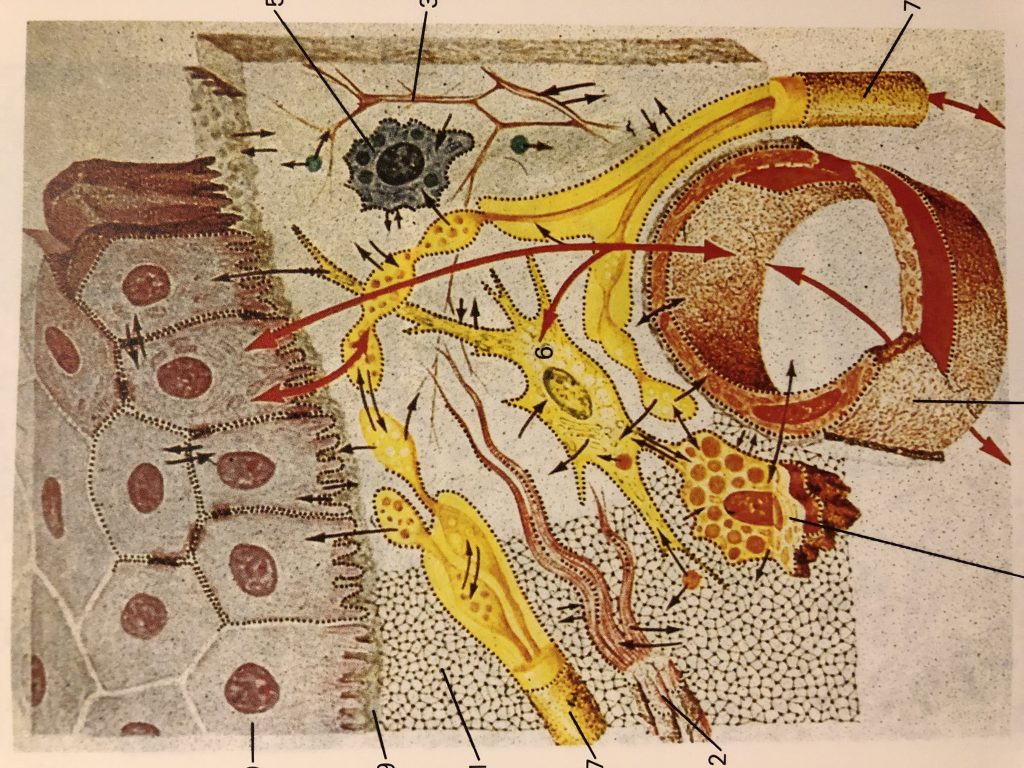
The epidermis is a host to keratinocytes, melanocytes
and immune cells such as Langerhans cells (LCs) and T lymphocytes, nerve-ending
cells (Merkel cells).The dermis is composed of an upper papillary (stratum
papillare) and lower reticular (stratum reticulare) dermis containing thin and
thick collagen fibers, respectively. The collagen fibers offer a mechanical
barrier as well as a structural environment
in which to host blood vessels and many immune cells such as dermal
dendritic cells (DDCs), ab T cells, gd T cells, natural killer (NK) cells, B
cells, mast cells, and macrophages can perform their function.
More recently, it was proposed a sentinel role in health
and disease for a spectrum of skin-resident cells ( with keratinocytes involved
in sensing pathogens and danger signals, migratory DCs capable of initiating a
diverse range of immune responses, and tissue-resident memory T (Trm) cells
performing crucial effector functions.
Skin-associated lymphoid tissue
(SALT) participates in trafficking of
immune cells between the skin, draining lymph nodes (LNs), and the peripheral
circulation (Streilein, 1983).
There is currently no vaccine to prevent coronavirus disease 2019 (COVID-19).
The best way to prevent illness is to avoid being exposed to this virus.
The virus is thought to spread mainly from person-to-person.
Between people who are in close contact with one another (within about 6 feet).
Through respiratory droplets produced when an infected person coughs or sneezes.
These droplets can land in the mouths or noses of people who are nearby or possibly be inhaled into the lungs.
Take steps to protect yourself
Clean your hands often
Wash your hands often with soap and water for at least 20 seconds especially after you have been in a public place, or after blowing your nose, coughing, or sneezing.
If soap and water are not readily available, use a hand sanitizer that contains at least 60% alcohol. Cover all surfaces of your hands and rub them together until they feel dry.
Avoid touching your eyes, nose, and mouth with unwashed hands.
Cover your mouth and nose with a tissue when you cough or sneeze or use the inside of your elbow.
Throw used tissues in the trash.
Immediately wash your hands with soap and water for at least 20 seconds. If soap and water are not readily available, clean your hands with a hand sanitizer that contains at least 60% alcohol.
Wear a facemask if you are sick
If you are sick: You should wear a facemask when you are around other people (e.g., sharing a room or vehicle) and before you enter a healthcare provider’s office. If you are not able to wear a facemask (for example, because it causes trouble breathing), then you should do your best to cover your coughs and sneezes, and people who are caring for you should wear a facemask if they enter your room. Learn what to do if you are sick.
If you are NOT sick: You do not need to wear a facemask unless you are caring for someone who is sick (and they are not able to wear a facemask). Facemasks may be in short supply and they should be saved for caregivers.
Clean and disinfect
Clean AND disinfect frequently touched surfaces daily. This includes tables, doorknobs, light switches, countertops, handles, desks, phones, keyboards, toilets, faucets, and sinks.
If surfaces are dirty, clean them: Use detergent or soap and water prior to disinfection.
To disinfect:
Most common EPA-registered household disinfectants will work. Use disinfectants appropriate for the surface.
Options include:
Diluting your household bleach.
To make a bleach solution, mix:
5 tablespoons (1/3rd cup) bleach per gallon of water
OR
4 teaspoons bleach per quart of water
Follow manufacturer’s instructions for application and proper ventilation. Check to ensure the product is not past its expiration date. Never mix household bleach with ammonia or any other cleanser. Unexpired household bleach will be effective against coronaviruses when properly diluted.
Alcohol solutions.
Ensure solution has at least 70% alcohol.
Other common EPA-registered household disinfectants.
Products with EPA-approved emerging viral pathogens pdf icon
[7 pages]external icon claims are expected to be effective against COVID-19 based on data for harder to kill viruses. Follow the manufacturer’s instructions for all cleaning and disinfection products (e.g., concentration, application method and contact time, etc.).
Spirulina is a blue green microalgae that grows in waters of subtropical climates.It is a type of cyanobacteria (cyano – blue pigment) that can be consumed as a superfood. Spirulina is has countless uses as a supplement for maintaining good health and preventing diseases. This is because it contains a plentiful supply of many important nutrients and antioxidants, including protein, complex carbohydrates, iron, and vitamins A and K, as well as B complex. It’s also rich in chlorophyll, fatty and nucleic acids, and lipids. Spirulina is rich in gamma-linoleic acid, or GLA, a compound found in breast milk that helps develop healthier babies. In fact it is often referred to as “Nature’s Multivitamin”.This is a breakdown of some of spirulina’s most significant benefits and nutrient composition.
Beta-Carotene
Spirulina contains powerful carotenoids such as best-carotene and yellow xanthophyll. It is one of the richest beta-carotene foods. The beta-carotene found in spirulina is ten times more concentrated than in carrots.
Iron
Spirulina is rich in iron, magnesium and trace minerals and is easier to absorb than iron supplements. And without the common side effects of iron supplementation.Ten grams of spirulina can supply up to 70% of the minimum daily requirements for iron.
Protein
About 60% of Spirulina’s dry weight is protein, which in the form it comes in within spirulina, is essential for growth and cell regeneration.
Gut Flora
Spirulina suppresses bad bacteria like E. coli and stimulates beneficial flora like lactobacillus and bifidobactria in the digestive tract to promote healthy digestion and proper bowel function.
Healthy flora is one of the foundations of good health. It increases the body’s ability to absorb nutrients from the foods we eat and helps protect against infection.
Detoxifier
Spirulina has a completely unique composition of phytonutrients, including chlorophyll, phycocyanin and polysaccharides, that can help to purge toxins from the body. In 1994, a Russian Patent was awarded for spirulina, deeming it a medical food for reducing allergic reactions from radiation sickness. This was a result of 270 children in Chernobyl consuming five grams a day for 45 days. Radionuclides were lowered by 50% and allergic sensitivities were normalized.
Cardiometabolic Benefits
Spirulina has been demonstrated to have cardiometabolic benefits – improving glycemic, lipid and blood pressure parameters.In a double-blind placebo controlled trial, overweight patients with hypertension were randomly allocated to receive 2g of Hawaiian spirulina daily for 3 months.The subjects that received spirulina exhibited a reduction in systolic blood pressure and some reduction in BMI (Body Mass Index).
Lipids
Spirulina also has a favorable effect on cholesterol.
A meta-analysis also showed that spirulina reduced plasma concentrations of total cholesterol, LDL and triglycerides.
Skin
Spirulina contains Vitamin E, selenium and tyrosine, which are all known for their powerful anti-aging effects.The antioxidants present in spirulina can aid in skin healing and support.
Quick Tip:
Adding 1-2 teaspoons of spirulina to your daily diet can be very beneficial.Try adding some to your smoothie or simply sprinkle a teaspoon into coconut water.
The flu, or influenza, is a viral illness that affects the respiratory tract including your nose, throat, lungs and bronchi. Mild cases of the flu can be confused with the common cold, however, the flu usually causes a more serious illness. Although it’s tempting to rely solely on natural remedies, the flu can be very serious, and one should always talk with a qualified healthcare provider if you think you may have the flu. Completely avoiding getting sick during the flu season ay be unrealistic, but there are ways to support your body naturally.The goal is to have a recovery plan and good sign of health is the recovery process itself.
Healing Herbs & Supplements
There are a variety of powerful supplements you can use as weapons against a flu virus.
Olive leaf is great for anyone who is starting to feel sick and noticing flu-like symptoms.
Echinacea and goldenseal are two supplements to incorporate when you are fighting a flu. Echinacea has been used for immune system support for hundreds of years.
Oregano is a great herb for flu viruses.Oregano oil is very powerful and should only be used short-term.
Elderberry syrup is another incredible flu-fighting supplement.
Elderberry (Sambucus nigra) is a herb that has a long history of use as a folk remedy for colds, sinus infections, and the flu. In preliminary lab studies, elderberry extracts have been found to fight off viruses. Researchers believe that anthocyanins, compounds found naturally in elderberries, may be the active component that strengthens the immune system and blocks the flu virus from sticking to our cells.
Propolis can be a powerful immune system support and can be great supplements to take if you start to feel the beginnings of a flu arise.
All different kinds of teas can provide benefits for someone suffering with flu symptoms. Steeping a strong cup of rose hips tea and adding in ample lemon juice can be particularly powerful and incredible for sore throats.Rosehips provide a great source of bioavailable Vitamin C. A simple lemon, honey & ginger tea provides soothing minerals to support you while you are healing.
Lots of rest & sleep.Sleep can help us immensely, it is very important for healing.
Hydration & lots of fluids. This is critical. Hydration allows the body to flush viral toxins out of the body and to keep the mucus thinned out. Staying away from heavy cooked foods is also helpful so that you don’t use up too much energy on digestion, which can instead be focused on healing.
Healing Foods & Recipes
Healing Broth
This healing broth is great while fighting off a flu. This healing broth can be nourishing, supportive, and help keep you from picking up any unwanted virus. Thus its useful to have all winter.
4 carrots, chopped or 1 sweet potato, cubed
2 stalks of celery, roughly chopped
2 onions, sliced
1 cup parsley, finely chopped
1 cup of shiitake mushrooms, fresh or dried (optional)
2 tomatoes, chopped (optional)
1 bulb of garlic (about 6-8 cloves), minced
1 inch of fresh ginger root
1 inch of fresh turmeric root
8 cups of water
Optional: Chili peppers or red pepper flakes
Place all the ingredients in a pot and bring to a boil. Turn heat down to low and allow to simmer for about an hour. Strain for a light soothing drink or leave the veggies in to enjoy as a light healing soup.
Congee
This simple rice soup is easily digested and assimilated, it harmonizes the digestion and is extremely nourishing.
1 cup rice, 1 garlic clove, 3 inch piece of ginger, 6 cups water.
Combine the rice, ginger, garlic and water in a large saucepan. Stir well. Cover and cook on low heat for approximately 1.5 hours until the rice is very soft and the congee has thickened.
Turmeric Ginger Garlic Orange Juice Shot
This is a powerful combination of flu fighting ingredients
2 oranges, 2 garlic cloves, 2 inch piece of turmeric, 2 inch piece of ginger
Run the ingredients through a juicer.Drink like a shot.This is a very powerful preparation.
Herbal supplements have been studied as supportive treatments for type 2 diabetes.
Type 2 diabetes affects more than 20 million Americans.It is a growing epidemic that is now very common and even seen in children. When someone has type 2 diabetes, it needs to be controlled through managing blood sugar levels. Diet and exercise are most important.
Herbal Supplements for Type 2 Diabetes
Several herbal supplements show promise in supporting type 2 diabetes.
Curcumin
The compound curcumin, which is found in the spice turmeric, has been shown to both boost blood sugar control and help prevent the disease. In a nine-month study of 240 adults with pre-diabetes, those who took curcumin capsules completely avoided developing diabetes while a sixth of patients in the placebo group did.
Ginseng
Ginseng has been used as a traditional medicine for more than 2,000 years. Studies suggest that both Asian and American ginseng may help lower blood sugar in people with diabetes. One study found that extract from the ginseng berry was able to normalize blood sugar and improve insulin sensitivity in mice.
Fenugreek
Benefits of fenugreek for diabetes have been demonstrated in both animal and human trials. In one study of 25 people with type 2 diabetes, fenugreek was found to have a significant effect on controlling blood sugar.
Cinnamomum verum(true cinnamon)
Consuming about half a teaspoon of this variety of cinnamon daily can result in significant improvement in blood sugar, cholesterol, and triglyceride levels in people with type 2 diabetes.
Aloe Vera
This plant has been used for thousands of years for its healing properties. Some studies suggest that the juice from the aloe vera plant can help lower blood sugar in people with types 2 diabetes.Aloe is available in juice form and can also be purchased fresh.The fresh leaves can be peeled and added to smoothies.
Milk thistle
This flowering herb is found around the Mediterranean See.Its active component is called silybinin. Milk thistle may reduce insulin resistance in people with type 2 diabetes who also have liver disease.
Holy basil (Tulsi)
This herb is commonly used in India as a traditional medicine for diabetes. Studies in animals suggest that holy basil may increase the secretion of insulin. A controlled trial of holy basil in people with type 2 diabetes showed a positive effect on fasting blood sugar and on blood sugar following a meal.
Gymnema
Gymnema has been used in traditional medicine as a treatment for diabetes. The Hindi name for this herb translates to “destroyer of sugar.”
Modern pharmacological research seems to support this traditional wisdom. Compounds extracted from gymnema have been shown to reduce the absorption of sugar from the intestinal tract and boost insulin production, all of which could help lower blood sugar. Furthermore, an active component of gymnema called gymnemic acid binds to the taste receptors on your tongue that perceive sweetness. As a result, it makes sweet things taste a lot less sweet.Animal testing confirms that gymnema reduces blood glucose levels.
Healing Foods Changing the diet is vital to managing Type 2 Diabetes.Eliminating processed foods, oils and sugars is critical, not only for diabetics, but for everyone.
Wild blueberries, papayas, blackberries, and raspberries are top fruits to eat if you have type 2 diabetes. Vegetables to focus on include spinach, celery, sprouts, kale, and asparagus. These foods help detoxify the liver, strengthen glucose levels, support the pancreas, boost the adrenal glands, and stabilize insulin.
Millions of adults around the world deal with hypertension or high blood pressure. Hypertension can be successfully managed through lifestyle modifications, medications, and natural remedies. Most people with hypertension experience improvement with prescription treatment and some may require more than one prescription medication to reach optimal blood pressure. Dietary modifications, exercise and smoking cessation are critical to managing hypertension, with or without the use of medication.Reducing alcohol and caffeine consumption as well as stress management are also important.
Herbal Remedies
Ginkgo Biloba – Ginkgo biloba can thin the blood while dilating your blood vessels, which allow the blood to circulate more easily, according to the University of Maryland Medical Center. This popular herb is also high in important antioxidants, which are known to lower blood pressure.
Hawthorn – Hawthorn supports the overall health of your cardiovascular system by strengthening the walls of the heart. This herb is a tonic for heart tissue.
Cinnamon – Specifically, Ceylon Cinnamon. Studies show that consuming cinnamon every day lowers blood pressure in those with diabetes.
Cat’s Claw – Traditional Chinese medicine has used cat’s claw to treat high blood pressure as well as neurological problems. Studies show that it can help reduce your blood pressure by acting on the calcium channels inside cells.
Celery – Chinese medicine has used celery seed for hundreds of years to treat high blood pressure, but juicing the entire plant has the same action. Celery is a known diuretic, which might be why it lowers blood pressure so effectively.
Black Cumin Seeds – Or Nigella seeds. Daily use of black cumin seed extract for 2 months may have a blood pressure-lowering effect in patients with mild hypertension according to studies. It also helps reduce LDL cholesterol levels, which is further beneficial for cardiac health.
Flax Seed – Rich in omega-3 fatty acids and Alpha-linoleic acid (ALA), which is the natural precursor of the cardio-protective long-chain n-3 fatty acids, flaxseeds protect heart health by reducing serum cholesterol, stabilizing blood pressure, and improving glucose tolerance. It’s also a potent antioxidant and so easy to add to any dish. According to research published in the European Journal of Clinical Nutrition, dietary supplementation with flaxseed oil (8d/day) lowers blood pressure. Another study found that there’s a significant reduction in both Systolic BP and Diastolic BP following supplementation with various flaxseed products. Since whole flaxseeds can pass virtually undigested through the human body, flaxseeds need to be freshly ground for best effect. Add 30 grams of freshly ground flaxseeds to your daily routine.
Recommended Foods for Heart Health (containing Antioxidants)
Cherries
Apricots
Oranges –Calcium protects the nervous system, Vitamin C
Wild blueberries (you can find these in the frozen section)
Raspberries
Blackberries
Mangos
Papayas
Watermelon
Zucchini
Broccoli
Asparagus
Kale
Artichokes
Pomegranate
Squash
Celery –contains bioavailable mineral salts –critical for everything in the body –fuel for the heart. Mineral salts conduct electricity. Magnesium. Potassium. Sodium.
Omega 3’s from Walnuts, hemp seeds, flax seeds, and chia seeds.
Chronic stress and anxiety affects millions of people. Nervousness, agitation, tension, racing heart, chest pain are just some of the overt symptoms these people experience. Anxiety is among the most common mental health issues. It has become an epidemic in the United States, so much so that it has overtaken depression as the leading mental health disorder. It is estimated that 40 million Americans struggle with anxiety.
Although there are many prescription medications that help treat the symptoms of anxiety, we may want to consider more natural remedies if a long-term solution is needed.
Exercise and Meditation
Exercise is a great way to burn off anxious energy, research and experience has demonstrated the effectiveness of exercise for many years. Talking walks in nature, gentle yoga and Qi Gong are all great ways to help manage anxiety symptoms long term.
Meditation is very effective in decreasing anxiety symptoms over time. Meditation can help to slow racing thoughts, making it easier to manage stress and anxiety. A meta-analysis combining the results of 163 different studies had an overall conclusion that practicing meditation produced beneficial results with significant improvement in anxiety. The easiest way to start is with guided meditations, which are available on YouTube and podcasts. A 5-minute daily meditation can have a profound effect with continued practice.
Lower sugar and processed food intake
Refined carbohydrates found in processed foods can create sugar highs and lows throughout the day. These highs and lows can trigger symptoms of anxiety. Processed foods can also cause mood swings and altered energy levels, making it potentially harder to manage anxiety symptoms. It is critical to avoid foods such as cakes, cookies, soda, fast foods, fried foods, processed meat, and refined grains when dealing anxiety.
Ashwagandha
This is one of the most revered herbs in Ayurvedic healing and is frequently referred to as the “Indian ginseng.” This is a rejuvenating herb that reduces anxiety without causing drowsiness, and helps stabilize the body’s response to stress.
Valerian root
Valerian naturally increases the amount of gamma aminobutyric acid (GABA) in the brain, which can calm anxiety. In fact, benzodiazepine medications work in a similar way.
Magnesium
Magnesium has many important roles in maintaining a healthy body, including calming the nervous system. It is also vital for GABA function. Interestingly, magnesium deficiency is a common deficiency in adults, so consider this supplement when recommending anti-anxiety treatment options. Magnesium glycinate is the best-absorbed form of magnesium and is the gentlest on the stomach. Topical magnesium preparations and Epsom salt baths are also a great option.
Vitamin B-complex
B vitamins help reduce stress and stabilize moods. Vitamin B6 should specifically be considered as a natural remedy for anxiety symptoms, because one of the signs of B6 deficiency is anxiety itself. Vitamin B6 helps to boost mood, balance blood sugar levels, and maintain a healthy nervous system.
Aromatherapy
Fragrant plant oils can help with stress and anxiety. Lavender essential oil is very helpful. A 2012 study tested the effects of aromatherapy with lavender on insomnia in 67 women aged 45–55. Results suggest that the aromatherapy may reduce the heart rate in the short term and help to ease sleep issues in the long term. To relieve stress, inhale 100% pure lavender essential oil straight from the bottle or apply it topically behind the ears, on the temples, and on the back of the neck. It is also safe to combine lavender essential oil with vetiver oil.
For stressful situations:
Rescue Remedy Gummies – take the heat off mild anxiety.
Lemon Balm Tincture (alcohol-free) knocks down anxiety. 3-4 droppers are great when you are up against confrontation.
Foods for healing Anxiety & Depression
Our diet can have a tremendous impact on our mental health. Try to incorporate a few of the following foods into your daily routine.
Cucumber Juice
Coconut Water
Lemon or Lime Water –great for electrolytes and neurotransmitters
Celery Juice –do it straight if you are dealing with anxiety and depression –gives mineral salts to build up electrolytes (16 ounces a day)
Wild Blueberries 1-2 cups daily. These are available frozen.
Spinach
Cilantro ½ cup daily
Spirulina 1-2 teaspoons daily
Lettuce
Winter Squash
Zucchini
Asparagus
Artichokes
Apples –an apple a day is great to alleviate anxiety & depression.
Information from Kerry Bone Principles of Phytotherapy
And Anthony William Medical Medium books.